





Delaware Health Alert Network #181
May 8, 2009 3:20 pm
Health
Update
DPH GUIDANCE FOR THE MEDICAL COMMUNITY IN DELAWARE REGARDING DIAGNOSIS AND TREATMENT OF SWINE
INFLUENZA:
UPDATED as of May 8, 2009
The recommendations in this Health Alert are based on the current situation and knowledge. Recommendations are changing quickly and this
Health Alert will be updated as necessary.
Situation
The Delaware Division of Public Health (DPH) is reporting 44 confirmed cases of swine-origin influenza A (H1N1) virus infection. The
onset of the first case was April 24. In addition, more than 500 symptomatic University of Delaware Students were treated for antiviral
agents at the University Health Center or a Division of Public Health clinic between April 29 and May 1.
The median age of confirmed cases is 19 years. 59% (26) of the cases are male. 55% (24) of the cases are known University of Delaware
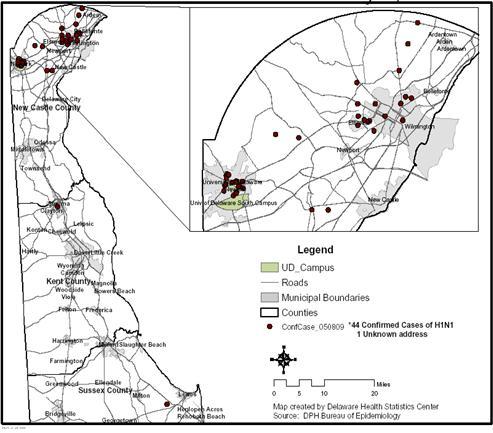
students. Only 2 cases have a known history of travel to Mexico. The epidemic curve and geographic distribution are below (Figures 1 and
2).
Figure 1 Date of Onset of Confirmed Cases of H1N1 Influenza, Delaware, Through May 8, 2009
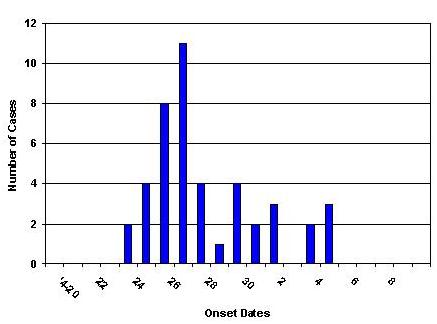
Figure 2 Confirmed Cases of H1N1 Influenza, Delaware, Through May 8, 2009
Surveillance of Influenza-Like Illness (ILI)
In addition to monitoring the epidemic in Delaware through laboratory confirmation of cases, DPH has implemented enhanced surveillance of
ILI. While not all components of enhanced surveillance are fully in place, they include:
- Sentinel day care centers – Surveillance system in development
- Sentinel nursing homes – No clear trend since May 4
- Chief complaint data from hospital emergency departments – Marked decrease since April 28
- Sentinel physician offices – No clear trend since May 1
- School absenteeism – Peak on May 1 then marked decrease
- Pharmacy drug usage – Surveillance system in development
- Major employers, Colleges and Universities – Qualitative reports indicate no ILI
Recommendations for Testing Suspect Cases
Not all people with suspected novel influenza (H1N1) infection need to have the diagnosis confirmed. Patients with symptoms that are not
severe can be treated empirically (see “Treatment” below).
Clinicians should test persons for the novel influenza (H1N1) virus if they have an acute febrile respiratory illness or sepsis-like
syndrome. Certain groups may have atypical presentations including infants, elderly and persons with compromised immune systems. Priority
for testing includes persons who 1) require hospitalization or 2) are at high-risk** for severe disease. To test for novel H1N1 influenza
virus, upper respiratory specimens, such as a nasopharyngeal swab or aspirate, nasal swab plus a throat swab or nasal wash, or tracheal
aspirate should be collected. Persons who perform nasal and tracheal
aspirate collections on ill persons require appropriate personal protective equipment.
For the purposes of disease surveillance only, DPH is seeking specimens from persons other than University of Delaware students with
influenza-like symptoms if they present with a fever >100° F and cough, sore throat, or nasal congestion.
Specimen storage and transportation information can be found here: http://www.dhss.delaware.gov/dph/php/alerts/dhan177.html
Recommendations for Treatment of Cases
Treatment is recommended for:
- All hospitalized patients with confirmed, probable or suspected novel influenza (H1N1).
- Patients who are at higher risk** for seasonal influenza complications
If a patient is not in a high-risk group or is not hospitalized, healthcare providers should use clinical judgment to guide treatment
decisions, and when evaluating children should be aware that the risk for severe complications from seasonal influenza among children
younger than 5 years old is highest among children younger than 2 years old. Many patients who have had novel influenza (H1N1) virus
infection, but who are not in a high-risk group have had a self-limited respiratory illness similar to typical seasonal influenza. For
most of these patients, the benefits of using antivirals may be modest, with efficacy decreasing significantly when administered past 48
hours of onset of symptoms. Therefore, testing, treatment and chemoprophylaxis efforts should be directed primarily at persons who are
hospitalized or at higher risk for influenza complications.
Chemoprophylaxis of contacts
Post exposure antiviral chemoprophylaxis with either oseltamivir or zanamivir can be considered for the following:
- Close contacts* of cases (confirmed, probable, or suspected) who are at high-risk** for complications of influenza
- Health care personnel, public health workers, or first responders who have had a recognized, unprotected close contact exposure to aperson with novel (H1N1) influenza virus infection (confirmed, probable, or suspected) during that person’s infectious period
(generally one day before and seven to ten days after onset of symptoms). Information on appropriate personal protective equipment is
available at: Interim Guidance for Infection Control for Care of
Patients with Confirmed or Suspected Swine Influenza A (H1N1) Virus Infection in a Healthcare Setting and might be updated frequently
as additional information on transmission becomes available.
Pre-exposure antiviral chemoprophylaxis should only be used in limited circumstances. Certain persons at ongoing occupational risk for
exposure who are also at higher risk** for complications of influenza (e.g., health care personnel, public health workers, or first
responders who are working in communities with influenza A H1N1 outbreaks) should carefully follow guidelines for appropriate personal
protective equipment or consider temporary reassignment.
* Close contact, for the purposes of this document, is defined as having cared for or lived with a person who is a confirmed,
probable or suspected case of novel influenza A (H1N1), or having been in a setting where there was a high likelihood of contact with
respiratory droplets and/or body fluids of such a person. Examples of close contact include kissing or embracing, sharing eating or
drinking utensils, physical examination, or any other contact between personslikely to result in exposure to respiratory droplets. Close
contact typically does not include activities such as walking by an infected person or sitting across from a symptomatic patient in a
waiting room or office.
** High-risk groups: A person who is at high-risk for complications of novel influenza (H1N1) virus infection is defined as the same
for seasonal influenza at this time. As more epidemiologic and clinical data become available, these risk groups might be revised.
- Children younger than 5 years old. The risk for severe complications from seasonal influenza is highest among children younger than
2 years old.
- Adults 65 years of age and older. Persons with the following conditions:
- Chronic pulmonary (including asthma), cardiovascular (except hypertension), renal, hepatic, hematological (including sickle cell
disease), neurologic, neuromuscular, or metabolic disorders (including diabetes mellitus);
- Immunosuppression, including that caused by medications or by HIV;
- Pregnant women;
- Persons younger than 19 years of age who are receiving long-term aspirin therapy;
- Residents of nursing homes and other chronic-care facilities.
More information:
- Delaware Health Alert Network and Press Releases: http://www.dhss.delaware.gov/dph/swineflucomm.html
- Delaware: http://www.dhss.delaware.gov/dph/
- Specimen storage and transportation: http://www.dhss.delaware.gov/dph/php/alerts/dhan177.html
- Clinicians: http://www.cdc.gov/h1n1flu/guidance/
- Identifying and Caring for Patients: http://www.cdc.gov/h1n1flu/identifyingpatients.htm
- Antiviral treatment: : http://www.cdc.gov/h1n1flu/recommendations.htm
- Laboratories: http://www.cdc.gov/h1n1flu/guidelines_labworkers.htm
- EMS: http://www.cdc.gov/h1n1flu/guidance_ems.htm
- General: : http://www.cdc.gov/swineflu/
For further information contact the Delaware Division of Public Health at (302) 744-4700.
Categories of Health Alert messages:
- Health Alert: Conveys the highest level of importance; warrants immediate action or attention.
- Health Advisory: Provides important information for a specific incident or situation; may not require immediate action.
- Health Update: Provides updated information regarding an incident or situation; unlikely to require immediate action.
